

Abstract
Background: Among youth with sickle cell disease (SCD), morbidity and mortality substantially increase following departure from pediatric care. Care continuity following transfer from pediatric to adult-centered care is paramount to ensure maintenance of health care delivery and reduce the risk of poor clinical outcomes. The American Academy of Pediatrics recommends matriculation in adult care within 6 months from leaving pediatric care for patients with special health care needs. Failure to transition from pediatric to adult care among youth with SCD may contribute to frequent disease complications and early death. No formal analysis has been conducted to quantify the risk of care interruption as youth transition from pediatric to adult care on the rate of acute health care utilization. We tested the hypothesis that patients who interrupted care for more than 6 months as they moved from the pediatric to the adult-centered care setting would have higher frequency of acute health care utilization.
Methods: With IRB approval, we conducted a retrospective review of the rate of acute care utilization among patients with SCD who were transitioned from the pediatric sickle cell program at St. Jude Children's Research Hospital to the adult sickle cell program at Methodist University Hospital, Memphis TN between January 2014 and December 2017. We compared the rates of emergency department (ED) and inpatient utilization among those who established care >6 months from completing pediatric care (interrupted care continuity) and those who established adult care within 6 months from completing pediatric care (uninterrupted care continuity). We used person-time rates to compare the rates of emergency department and inpatient encounters per patient between the two care continuity groups.
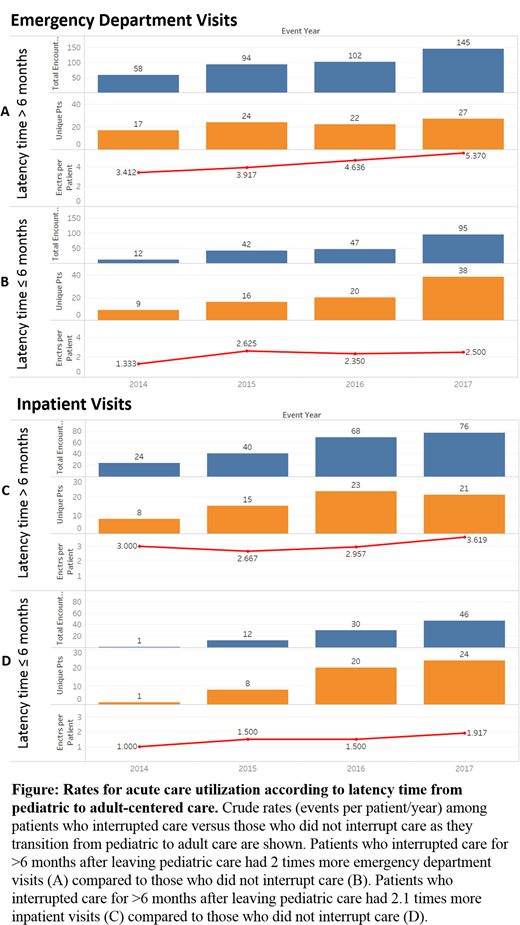
Results: Between January 2014 and December 2017 there were 172 patients with SCD who completed pediatric care and established adult care: 63 of them had a latency time from pediatric to adult care >6 months and 109 had a latency time from pediatric to adult care ≤6 months. Their follow-up since matriculation in adult care was 2245 and 2197 person-years for interrupted and uninterrupted care continuity groups, respectively The median (range) age upon establishing adult care was 20 (range, 20 to 24) years and 18 (range, 18 to 19) years for the interrupted and uninterrupted care continuity groups, respectively. Patients who interrupted care >6 months after leaving pediatric care had an incidence rate of 0.18 ED visits/person-year compared to 0.09 ED visits/person-year among those who completed the first visit within 6 months from leaving pediatric care (IRR 0.48, 95%CI 0.40-0.57, p<0.0001) (Figure panels A and B). Patients who interrupted care >6 months after leaving pediatric care had an incidence rate of 0.09 inpatient visits/person-year compared to 0.04 inpatient visits/person-year among those who completed the first visit within 6 months from leaving pediatric care (IRR 0.42 (95%CI 0.32-0.54, p<0.0001) (Figure panels C and D).
Conclusions: The latency time from pediatric to adult care may impact the frequency of acute care utilization among youth with SCD. Patients who do not establish adult care within 6 months from leaving pediatric care, as recommended by the American Academy of Pediatrics, are at risk of experiencing greater ED and inpatient visits than those who establish care within 6 months from leaving pediatric care. Efforts to avoid care interruptions during the health care transition period are important to ensure optimal health outcomes among youth with SCD.
Hankins:NCQA: Consultancy; bluebird bio: Consultancy; Novartis: Research Funding; Global Blood Therapeutics: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal